FAQ
Published by: https://fastlifehacks.com/n95-vs-ffp
Masks vs Respirators
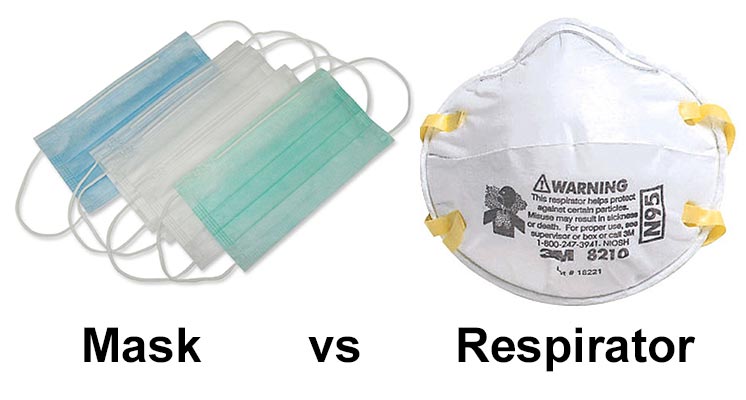
Before we go any further, lets just clarify on a technical difference between a “mask” and a “respirator”. In day to day language we often say mask, when referring to what are technically called respirators.
Uses for Masks:
- Masks are loose fitting, covering the nose and mouth
- Designed for one way protection, to capture bodily fluid leaving the wearer
- Example – worn during surgery to prevent coughing, sneezing, etc on the vulnerable patient
- Contrary to belief, masks are NOT designed to protect the wearer
- The vast majority of masks do not have a safety rating assigned to them (e.g. NIOSH or EN)
Uses for Respirators:
- Respirators are tight fitting masks, designed to create a facial seal
- Non-valved respirators provide good two way protection, by filtering both inflow and outflow of air
- These are designed protect the wearer (when worn properly), up to the safety rating of the mask
- Available as disposable, half face or full face

Respirator Standards
Whilst surgical style masks are not redundant by any means (discussed more below), they aren’t designed to protect the wearer, whilst respirators are.
The US Center for Disease Control (CDC) cites the N95 respirator standard as part of the advised protective equipment in their Covid-19 FAQ and their SARS guidance (SARS being a similar type of Corona virus). Which suggests that an N95 or better respirator is acceptable.
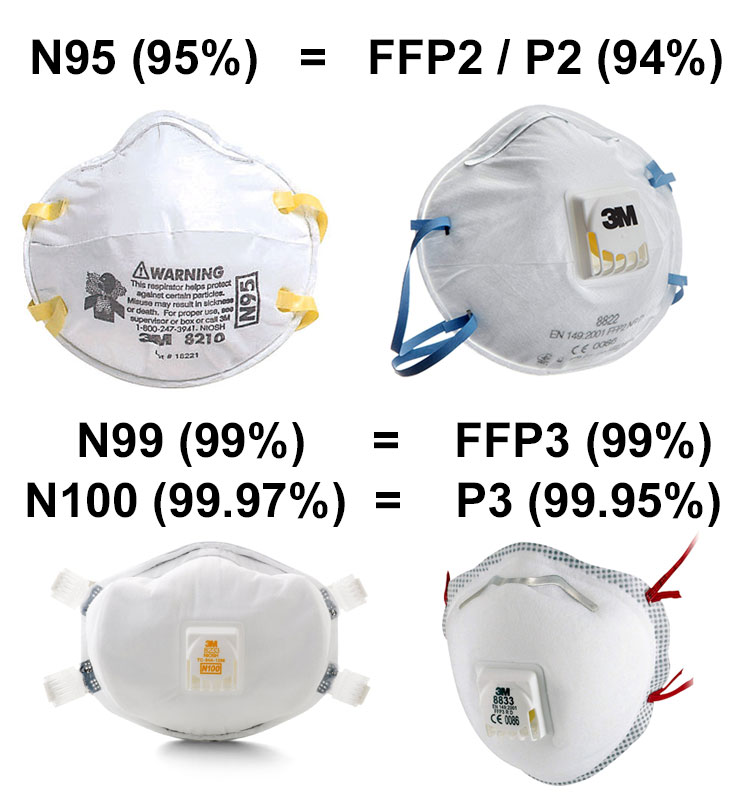
N95 vs FFP3 & FFP2
The most commonly discussed respirator type is N95. This is an American standard managed by NIOSH – part of the Center for Disease Control (CDC).
Europe uses two different standards. The “filtering face piece” score (FFP) comes from EN standard 149:2001. Then EN 143 standard covers P1/P2/P3 ratings. Both standards are maintained by CEN (European Committee for Standardization).
Let’s see how all the different standards compare:
| Respirator Standard | Filter Capacity (removes x% of of all particles that are 0.3 microns in diameter or larger) |
|---|---|
| FFP1 & P1 | At least 80% |
| FFP2 & P2 | At least 94% |
| N95 | At least 95% |
| N99 & FFP3 | At least 99% |
| P3 | At least 99.95% |
| N100 | At least 99.97% |
As you can see, the closest European equivalent to N95 are FFP2 / P2 rated respirators, which are rated at 94%, compared to the 95% of N95.
Similarly, the closest to N100 are P3 rated respirators – with FFP3 following closely behind.
You could approximate things to say:
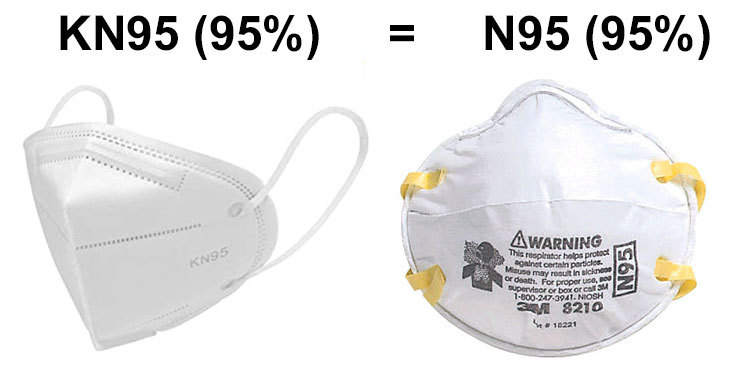
KN95 vs N95
Yes. N95 has the same specification as the Chinese KN95. See 3M document (link) – to quote “it is reasonable to consider China KN95, AS/NZ P2, Korea 1st Class, and Japan DS FFRs as equivalent to US NIOSH N95 and European FFP2 respirators”
Things to watch out for:
- No guarantee that all KN95 respirators meet the KN95 standard – watch out for scams
- Also look out for – good seal around face / some padding for comfort / tie around face straps with adequate strength and tension
Are N95/N100 actually better than FFP2/P3?
Not neccessarily, it’s important to note that these standards only specify the minimum % of particles that the respirator filters. For example, if a mask is FFP2 rated, it will filter at least 94% of particles that are 0.3 microns in diameter or larger. But in practice it will filter somewhere between 94% and 99%. The precise figure will often be quoted by the manufacturer in the product description.
A good example is the GVS Elipse respirator, which in the USA (link) is rated at P100 (99.7%), and in Europe (link) is rated at P3 (99.95%). In practice it’s likely to have the same filtering capacity in both regions.

Valve vs Non-Valved Respirators

Valved respirators make it easier to exhale air. This makes them more comfortable to wear, and leads to less moisture build-up inside the respirator. Ideal for things like DIY/construction work.
The problem with valved respirators is that they do not filter the wearer’s exhalation, only the inhale. This one-way protection puts others around the wearer at risk, in a situation like Covid-19. It’s for this reason that hospitals and other medical practices do not use valved respirators.
TL;DR – yes, respirators with high efficiency at 0.3 micron particle size (N95/FFP2 or better) can in theory filter particles down to the size of the coronavirus (which is around 0.1 microns). What that doesn’t tell us is how much protection respirators will provide against coronavirus when in use – we will need to wait for future studies to confirm.
Read on to learn more…
A recent paper shows that the coronavirus ranges from between 0.06 and 0.14 microns in size. Note that the paper refers to the coronavirus particle as 2019-nCoV, which was it’s old name. The virus is currently called SARS-CoV-2, and the illness it presents in people is called Covid-19.


Respirator’s are measured by their efficiency at filtering particles of 0.3 microns and bigger (noting that the coronavirus is smaller than that).
The reason for the focus on 0.3 microns is because it is the “most penetrating particle size” (MPPS). Particles above this size move in ways we might anticipate, and will get trapped in a filter with gaps smaller than the particle size. Particles smaller than 0.3 microns exhibit what’s called brownian motion – which makes them easier to filter. Brownian motion refers to a phenomenon whereby the particle’s mass is small enough that it no longer travels unimpeded through the air. Instead it interacts with the molecules in the air (nitrogen, oxygen, etc), causing it to pinball between them, moving in an erratic pattern.
According to researchers this point between “normal” motion and brownian motion is the hardest particle size for filters to capture.
What we can take away from this, is that high filter efficiency at 0.3 micron size will generally translate to high filter efficiency below this size also.
For more discussion and details on the subject of respirator filters and brownian motion – see this great post at smartfilters.com.

Now lets look at specific research that measures the filter efficiency at 0.3 microns and below (coronavirus territory)…
- This article by 3M discusses research showing that all 6 of the N95 respirators they tested can efficiently filter lower than 0.1 micron size with approximately 94% efficiency or higher. The graph below is from that article, and illustrates this:

- Additionally, smartfilters.com have a great article on this subject, citing research showing that the respirators tested could filter down to 0.007 microns (much smaller than Covid-19). For example the 3M 8812 respirator (FFP1 rated) was able to filter 96.6% of particles 0.007 microns or larger. Suggesting FFP2 or FFP3 would achieve even greater filtration.
The below image (click it to expand) shows the size of the coronavirus, relative to other small molecules like a red blood cell, or the often talked about PM2.5 particle size.

Image of coronavirus vs other particles – from smartairfilters.com
Risks With Using Respirators
There are a number of possible risks with respirators that it’s worth being aware of, so that you can avoid making them.
- Not fitting and wearing respirators correctly – A respirator can’t fully protect you if it doesn’t fit your face. See OSHA guidance on fit testing and fit checking for more info.
- Touching the front of the respirator (which catches viruses etc) and then transferring that to other objects, which could eventually lead back to your mouth and nose.
- Taking unnecessary exposure risks because you’re wearing a respirator. Don’t let it give you false confidence. The safest thing is maintaining social distance.
For further discussion on these 3 points, see the expandable box below:
Reliable Brands?
For those in the UK, three of the more reliable brands are 3M, JSP and GVS. All carry the CE mark and offer FFP ratings.
Similarly in the USA, 3M and GVS are reliable, offering both N95 and N100 ratings.
For those outside the UK or USA, look for brands that carry ratings appropriate to your country. For example, China has a KN95 standard which uses China GB2626-2006 standard, and is almost identical to N95 standard. See this 3M PDF for more details on other standards (including Korea and Japan).
Respirator Re-Use – How to sanitize them safely?
Research from SmartAirFilters (link) showed that after 11 days of heavy use in polluted Beijing, their respirator had only lost 1.4% of filtering capacity. So we know that disposable respirators can continue to function for more than 1 day/1 use – fortunately!

What isn’t so clear however, is how to sanitize respirators safely, without destroying the filtering function. Research gathered from various sources, suggests the following methods are either good or bad:
| Better Decontamination Options | Worse Decontamination Options |
|
|
|
|
|
|
|
|
|
|
|
*There’s a lot to discuss here, and so it needs a separate post. Read more about it here:
– Respirator Re-Use – How to sanitize them safely?
Surgical Masks
Surgical masks are generally speaking a 3-ply (three layer) design, with 2 sheets of “non-woven” fabric sandwiching a “melt-blown” layer in the middle. It’s the melt-blown layer that provides the filtering capability. A melt-blown material is also used in respirators, and thus you can imagine it’s more expensive and hard to come by recently, due to demand.

Image of the melt-blown filaments under microscope come from mdpi.com
The melt-blown fabric is made by melting a plastic, then blowing it from either side at high velocity onto a rotating barrel. Done right, this results in a fabric composed of tiny filaments. For a more technical (!) explanation of the process – see here.

Diagram of melt-blown machinary (left) comes from Erdem Ramazan’s book, and the image of melt-blowing in progress (right) comes from 4FFF on wikipedia
Not all melt blown fabric has the same filtering capability, some are better than others. Unfortunately we can’t test the filtering capability of the melt-blown layer without specialized knowledge and equipment. What we can do, however, is at least check that the melt-blown layer is present.
Below I show an example of a surgical mask (left) that came without the melt-blown layer. You can imagine that, given the extra cost and current scarcity of melt-blown fabrics, manufacturers might cut corners with this layer, so it’s worth keeping an eye on.

Choosing surgical masks that have been tested according to a set of standardized test methods (ASTM F2100, EN 14683, or equivalent) will help avoid low quality products. The ASTM standard for surgical masks (particularly levels 2 & 3) are primarily focused around fluid resistance during surgery. These higher levels don’t offer much extra in the way of protection from Covid-19 under non-surgical conditions.

Whilst FFP2/FFP3 or N95/N100 are the gold standard as far as face protection goes, what about surgical masks, do they provide any protection?
Strictly speaking, surgical masks are primarily designed to protect vulnerable patients from medical professionals. Stopping the wearer (e.g. surgeon) from spreading their germs when coughing/sneezing/speaking. So they’re designed to protect patients, not to protect the wearer.
An obvious flaw with surgical masks compared to respirators is their lack of a tight face fit, which leaves gaps around the edges.
There isn’t currently research available on the efficacy of surgical masks (or even respirators), for protecting wearers against the coronavirus. Although this isn’t totally surprising given how new the virus is.
In lieu of that, the below looks at research around the use of surgical masks and N95 masks in the context of influenza, looking specifically at the protection given to the wearers. Influenza may be a good virus particle to compare it to, as they are both transmissible through droplets and aerosol, both cause respiratory infection, and both are similar in particle size.
N.B. Please don’t conflate the comparison to the influenza particle as suggestion that they are comparable illnesses – current data suggests that the coronavirus may have a higher mortality rate.

Source for coronavirus (SARS-CoV-2) size is this paper, whilst sources for Influenza size are this paper (eventually published in Vaccine), and a Frontiers in Microbiology paper.
In the first study we will look at, 2,862 US health care personnel were split into 2 groups, those wearing N95 masks and those wearing surgical masks1. There were 207 lab confirmed influenza events in the respirator wearing group, compared to 193 in the mask wearing group – a difference that was not statistically significant.

In the next study, Canadian nurses were split into 2 groups, those wearing N95 masks and those wearing surgical masks. There were 50 cases of influenza in the surgical mask group, compared to 48 in the N95 respirator group2. Again, no significant difference.

So where does this leave us? Those 2 studies suggest that surgical masks are approximately comparable to N95 masks when it comes to preventing influenza illness in close contact clinical settings. What this doesn’t tell us, is whether they’re better than wearing nothing on our faces.
To find that out, we need a study that has a control group that doesn’t use any facial protection. Due to ethical considerations, those studies aren’t abundant, but we do have at least one.
In this Australian study, they looked at 286 adults in 143 households who had children with influenza-like illness3. For clarity, influenza-like illness is not the same as laboratory confirmed influenza. It’s diagnosed by symptoms like fever, dry cough and feeling sick, which could mean influenza, but could also be caused by the common cold or other viruses. They found that adults who wore masks in the home were 4 times less likely than non-wearers to be infected by children in the household with a respiratory infection. There is nice analysis of the study here by Imperial College London.

Image via smartairfilters.com
It’s definitely fair to note that this Australian study was very small, and could not be considered definitive by any means. That being said, we’ve got to work with what he have, and this at least gives us some data points:
- Wearing a surgical mask or N95 (FFP2) respirator was better (in the study) at protecting against influenza-like illnesses than wearing nothing at all
- Whilst we can anticipate surgical masks to be inferior to respirators, the studies above suggest they are not as inferior as one might assume. For example the first two studies didn’t find a significant difference between surgical masks and N95 respirators, when protecting wearers against influenza.
- Important to note that we’ve used influenza protection as a proxy for SARS-CoV-2 (coronavirus). This is done because SARS-CoV-2 is new and there are no comparable studies on it. But of course the drawback is that it still leaves a lot of uncertainty, as SARS-CoV-2 may act quite differently in terms of transmission.
In a lab setting, with artificial conditions, we find that surgical masks are able to block 80% of particles down to 0.007 microns. Compared to the 3M 8812 respirator in this study which blocked 96% (FFP1 rated). This generally aligns with our discussion above.

Image via smartairfilters.com
In conclusion: we don’t know how much protection surgical masks provide against the novel coronavirus. However, the above at least suggests that a surgical mask may provide more than zero protection – and that’s worth being aware of. It makes sense to only wear them for protection as a method of last resort – with respirators being the primary choice.
Is is much safer to avoid the company of people who are sick or potentially sick, and to reduce social contact overall, especially to large groups of people (see the social distancing section below). To repeat, the use or surgical masks would have to be a last resort – and wearing one should not encourage anyone to take unnecessary exposure risks.
If we are in the presence of someone sick, who has/might have the coronavirus, it makes sense for them to wear a mask or respirator to reduce their ability to spread the disease.
DIY / Homemade Masks
The CDC has recently announced guidance to American citizens that “cloth face coverings” should be used in public settings where social distancing measures are difficult to maintain. Noting that surgical masks and N95 respirators should be reserved for healthcare workers. If citizens don’t buy respirators or surgical masks, they’re left to buy fabric based masks from places like Amazon (yes, they do have some), or, they need to make their own.

Image from the masks4all.co DIY mask project
So how does one make their own mask?
Firstly, it’s worth noting how various household items compare in terms of filter efficacy and breathability. For that, we can refer to a Cambridge University study (link), which revealed “the pillowcase and the 100% cotton t-shirt were found to be the most suitable household materials for an improvised face mask”.

Image via SmartAirFilters
Interestingly, other items such as vacuum cleaner bags and dish towels showed greater filtration capacity, so why didn’t the study pick them? Unfortunately those items performed badly in the breathability tests. A mask is little good if you can’t breathe out of it. See this write-up of the study for more details (and nice graphs!)
Below are some DIY mask methods, listed from simple to advanced:
1) No modifications T-Shirt Mask
Don’t want to get the scissors out? No problem. This method shows how to wrap a T-shirt around your face without adjusting it. Based on the above study, use 100% cotton t-shirts where possible. Find the full guide for this method here.

2) No Sew T-Shirt Mask
This method uses just a t-shirt, scissors, pen and ruler. View the full instructions on Runa Ray’s YouTube video.

3) Sewing Machine Required Masks
For those with sewing machines… 2 good mask tutorials come to mind. The first, a simple one (YouTube link), the second – a more advanced design with ties, fitted nose and filter pocket (YouTube link).

Of course, it *hopefully* goes without saying that the level of protection these DIY masks offer is below that of surgical masks and respirators.
If you’ve seen other great DIY mask designs, please share them below in the comments.
What are respirators protecting us against?
Droplets
A primary reason for wearing a respirator is to protect from droplets. For example if a sick person coughs or sneezes when in close proximity to us, the respirator forms a barrier to prevent their bodily fluids reaching our face.
Droplets are generally large, and gravity drags them down to land on objects, rather than staying in the air. So they don’t travel very long distances. There is however research into micro droplets, which get ejected even during talking. This Vimeo video made by Japanese researchers, captures micro droplets on video using high speed cameras. We know large droplets play a role in transmission, but it’s not yet clear what role micro droplets play.

Image from Sui Huang’s blog post on the need for mask usage
Aerosols
What may remain in the air for some time are aerosolized virus particles. So for example, you could imagine someone creating two issues when sneezing, the first are ejected droplets, which travel a short distance, then second, aerosolized virus particles that stay in the air for longer.
Currently there is debate and uncertainty around how long Covid-19 can remain aerosolized, and how much of a risk that vector is compared to others.
What we can do is be aware of what research currently says, and err on the side of caution until its been confirmed.
Scientists at the National Institute of Allergy and Infectious Diseases (NIAID) published a study in NEJM (link) on what can happen under controlled lab conditions. They used a nebulizer, which creates an aerosol from liquids, and tested how long the virus remains measurable in the air whilst aerosolized. They also tested how long the virus was measurable on other surfaces. Their results showed the virus remained measurable for the full duration of the aerosolization experiment; 3 hours. See the graphs below for more details:

This image comes from the NIAID pre-print discussed above, showing the virus titer (viral load)
Dr John Campbell has made a YouTube video discussing this paper in more detail.
Mouth & Nose
Then lastly, whilst the respirator covers our face, it makes it very hard for us to touch an object with the virus and transfer it to our mouth and nose. This is a kind secondary benefit, in addition to the two mentioned above. We just need to make sure we wash our hands carefully as soon as we take the respirator off.
Is Eye Protection Necessary?

Whilst the coronavirus can’t penetrate skin, it can penetrate all exposed mucous membranes, which includes the eyes.
This is why you often see medical professionals wearing eye masks when in contact with infected patients.
That said, eyes are presumably a lower risk as a route of entrance, compared to the mouth, which is constantly breathing air directly into the lungs.
For eye protection, there are two routes that people go down; one is a disposable respirator and safety goggles, the other is a full face respirator. Safety goggles with a rubber air seal provides a tighter air barrier. For example, Bollé make some minimalist models which include a rubber seal, but there are many options available.

Related Questions…
What can you do to reduce risk?
Social Distancing
Viruses like the flu and novel coronavirus are spread by people who have the virus coming in to contact with people who are not infected.
The more you come in to contact with infected people, the more likely you are to catch the infection.
Social distancing, according to Wikipedia, are infection control actions that are taken by public health officials to stop or slow down the spread of a highly contagious disease.
We are seeing this in action already in countries such as China, South Korea and Italy.
In addition to social distancing measures taken by governments, we can ourselves choose to reduce physical exposure to potentially sick people, for example:
- Exploring the option to work from home if your job allows for it.
- Avoiding large public gatherings such as sporting events or situations where you may come in to contact with crowds of people (such as shopping malls, gyms or cinemas)
- Interacting with people over the phone/video calls, instead of in person.
These types of steps may be an impediment to normal life. However, the intention is that these will be a short term measure – not forever!
One of the main risks with a pandemic is that the initial spread is so quick that it overwhelms the health services. A key aim for any country should be to avoid that, and social distancing can help.

Avoiding crowded places (such as packed trains) may be necessary to reduce spread
Regular Hand Washing
– The CDC recommend regular hand washing with soap and water for at least 20 seconds.
– Prioritize washing prior to eating and after being out.
– Regular hand washing dries the hands, which at an extreme, may make them vulnerable to infection. To mitigate this, regularly use a glycerin based moisturizer with pump or squeeze mechanism. Those that you scoop are less hygienic.
– A study showed that we touch our face on average 15x per hour. That behaviour may be difficult to change, but if we keep our hands clean, it’s less detrimental.

Image showing the differences in effect between types of hand washing.
Trim Finger Nails
Short finger nails reduce the risk of trapping dirt (and viruses) under the nails. One method to check if your nails are too long is by putting them against your palm. If you can’t feel your fingers but just nails, then they are too long to be kept clean easily.

Alcohol Based Hand Sanitizer
– The CDC recommend that if soap and water are not available, use an alcohol-based hand sanitizer with at least 70% alcohol. Leave to air dry.
Sanitize your phone
– Given how often we use our phones, this seems like the next logical priority to be sanitized. Using antibacterial wipes or alcohol swabs (typically 70% alcohol) to clean your phone and other items is a good option. If the antibacterial wipes claim to be able to kill the flu virus (H1N1) – that’s a good sign they may be able to do similar for the coronavirus. Once finished wiping, leave to air dry.
Be aware of other items you touch regularly, including:
- Computer keyboard and mouse
- House and car keys
- Re-usable water bottles
- Car steering wheel
- Clothing pockets
- Door handles
And take appropriate caution when interacting with them – sanitizing where possible.

Keep your immune system healthy
Examples of action you can take to maintain a healthy immune system:
Sleep
Get adequate, high quality sleep. For most people ‘adequate’ means 7-8 hours. It’s no coincidence that “burning the candle at both ends” increases risk of illness. A 2004 literature review concluded that “sleep deprivation has a considerable impact on the immune response” and “should be considered a vital part of the immune system”4
Exercise
Exercise regularly, but don’t overdo it. To quote a 2007 study on exercise and the immune system – “moderate exercise seems to exert a protective effect, whereas repeated bouts of strenuous exercise can result in immune dysfunction”5.
Vitamin D
There is evidence suggesting:
- Vitamin D plays a key role in immune function
- Being deficient in vitamin D can make you more susceptible to infection
- Vitamin D supplementation protects against acute-respiratory tract infections
- Whilst noting that none of this relates specifically to the coronavirus, but is about general healthy immune function

From a British Medical Journal meta-analysis (link), covering 25 randomized controlled trials (11,321 participants).

From a British Medical Journal article on Vitamin D and the immune system (link)
We can get vitamin D from our diet (small amounts) and from sun exposure. If you’re not getting much sun, it can be difficult to get adequate amounts of vitamin D from the diet alone.
What is an adequate amount of vitamin D? The National Institutes of Health (NIH) suggest getting 600iu (15mcg) from all sources, per day, for adults. Similarly the National Institute for Health and Care Excellence (NICE) suggest a supplement containing 400iu (10 micrograms) taken daily.
Dr John Campbell has a great video on vitamin D and the immune system . He cites the NICE guidelines of supplementing 400iu per day, and says he personally takes a vitamin D supplement containing 1,000iu daily.
When looking for a supplement, there is evidence to suggest (link) that vitamin D3 raises levels of vitamin D with 1.7x greater efficiency than D2. Examples of NSF certified manufacturers selling vitamin D3 are Life Exension – 1,000iu, Thorne Research – 1,000iu and Pure Encapsulations – 1,000iu.

Roundup
Hopefully if you’ve stumbled across this article, and you were confused about the difference between N95, KN95 and FFP2/FFP3 masks, this has cleared things up for you.
For Spanish speaking friends who might find this article useful, it’s translated here.
If you have any further questions, please leave them below in the comments.
Further Learning
For preventative measures you can take as an individual (which also benefits the collective) see this short list of videos by Dr John Campbell:
- Vitamin D and the immune system – YouTube video
- Fevers – good or bad? Hint: often very good – YouTube video part 1 and part 2
- How to avoid viruses around us (including cleaning tips) – YouTube video
- How long Covid-19 stays viable and dangerous on surfaces and in the air – YouTube video

Dr John Campbell on YouTube
See Post Sources Below:
- N95 Respirators vs Medical Masks for Preventing Influenza Among Health Care Personnel – A Randomized Clinical Trial – Lewis J. Radonovich Jr, MD et al. – JAMA – Sept 2019
- Surgical Mask vs N95 Respirator for Preventing Influenza Among Health Care Workers – A Randomized Trial – Mark Loeb et al. – JAMA – Nov 2009
- Face Mask Use and Control of Respiratory Virus Transmission in Households – MacIntyre et al. – Emerging Infectious Diseases Journal – Feb 2009
- Sick and tired: does sleep have a vital role in the immune system? – Bryant et al. (2004)
- Exercise and the Immune System – Brolinson (2007)